Cardiovascular complications remain a leading cause of early mortality after liver transplantation and major hepatic resection, yet the molecular pathway linking hepatic injury to remote cardiac damage has long remained elusive. A new study from Beijing Tsinghua Changgung Hospital, Tsinghua University, identifies circulating ATP released from the ischemic liver as the initiating signal that drives remote cardiac injury through cardiac macrophage inflammasome activation.
Led by Prof. Zhifeng Gao, Director of the Department of Anesthesiology at Beijing Tsinghua Changgung Hospital, in collaboration with Prof. Dan Lu’s group at the Institute of Systems Biomedicine, School of Basic Medical Sciences, Peking University, the team integrated a 382-patient clinical cohort, a murine hepatic ischemia-reperfusion (HIRI) model, and cardiac immune single-cell transcriptomics to delineate the liver-to-heart injury cascade, and identified the ATP-P2X7/adenosine-A2A purinergic axis as a potential pharmacological target for perioperative cardioprotection.
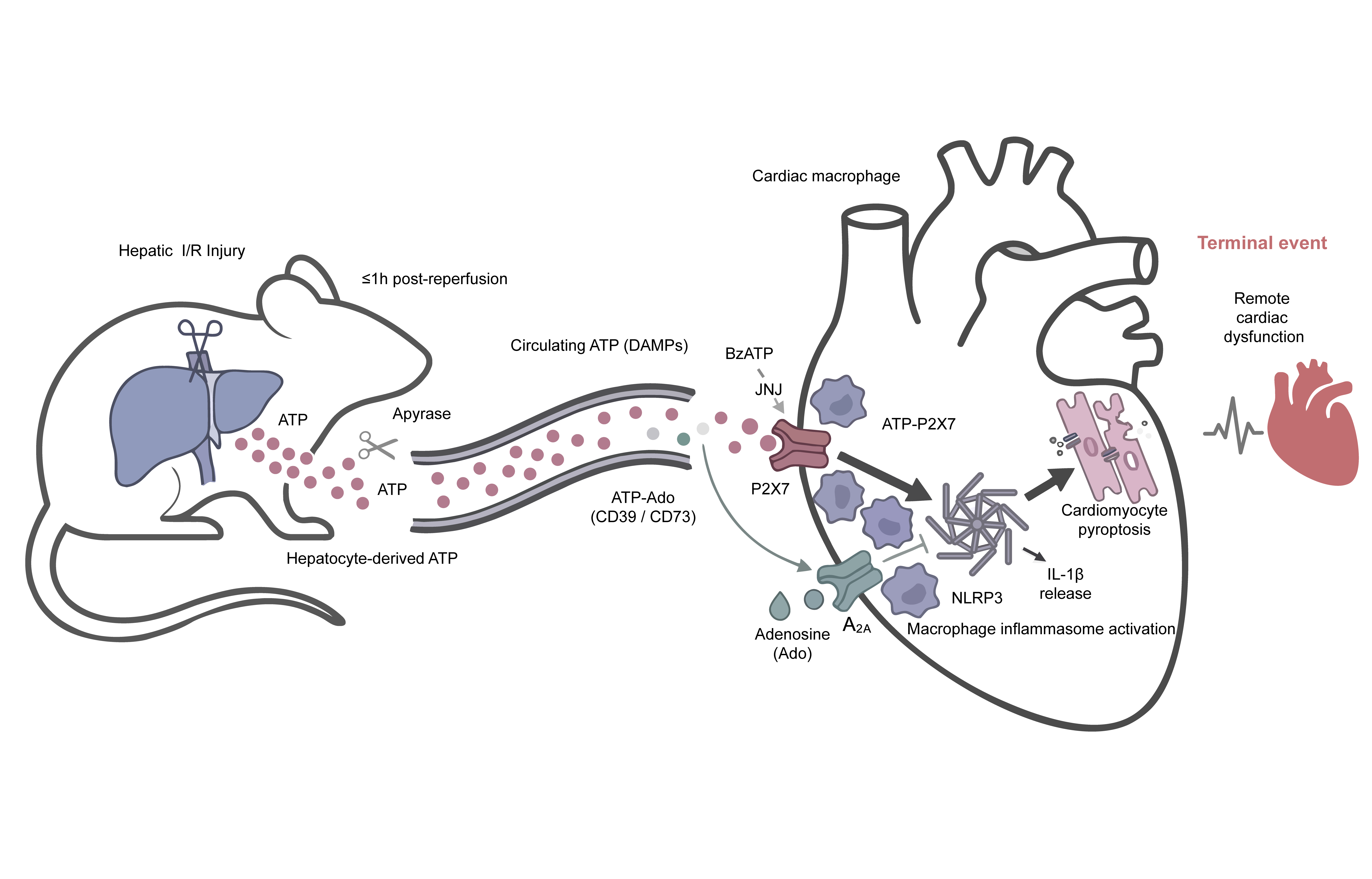
Schematic overview: liver-derived ATP drives remote cardiac injury via macrophage P2X7-NLRP3 inflammasome activation
The study first established a graded clinical association between hepatic and cardiac injury, then validated causal drive in animal models. Among 382 patients undergoing elective hepatic resection, the incidence of myocardial injury after noncardiac surgery (MINS) rose from 20.5% to 50% across ascending peak postoperative ALT strata (P<0.0001), accompanied by prolonged hospital stay and elevated ICU admission. In mice, plasma ATP surged within one hour of reperfusion, well before cardiac troponin rose. A vascular ATP gradient from the portal vein to the inferior vena cava to the left ventricle, together with depleted hepatic ATP stores, identified the ischemic liver as the principal source. Intravenous ATP injection into naive mice recapitulated cardiac injury, whereas enzymatic clearance of circulating ATP preserved cardiac function, together satisfying the criteria of both sufficiency and necessity.
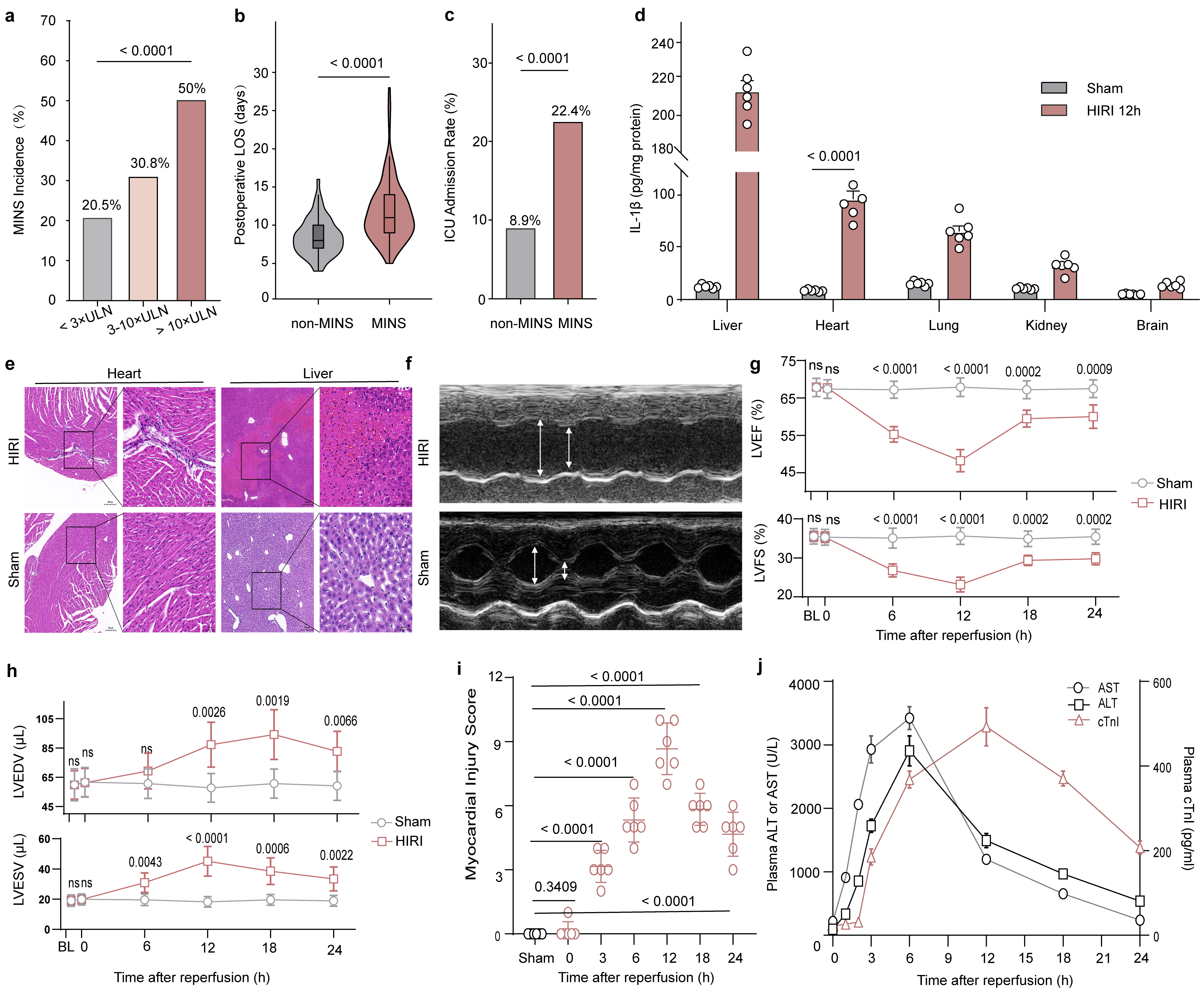
Clinical cohort and murine model jointly demonstrate that hepatic injury drives remote cardiac injury
Single-cell transcriptomic profiling of cardiac immune cells revealed that monocyte-derived macrophages (MoMF) already resident in the steady-state heart underwent inflammatory reprogramming after HIRI, with coordinate upregulation of P2X7, NLRP3, and IL-1β; tissue-resident macrophages showed minimal expression of these inflammasome components. This finding extends the prevailing CCR2+ monocyte recruitment paradigm derived primarily from myocardial infarction studies, indicating that pre-existing cardiac MoMF can undergo in situ inflammatory reprogramming in response to distant danger signals.
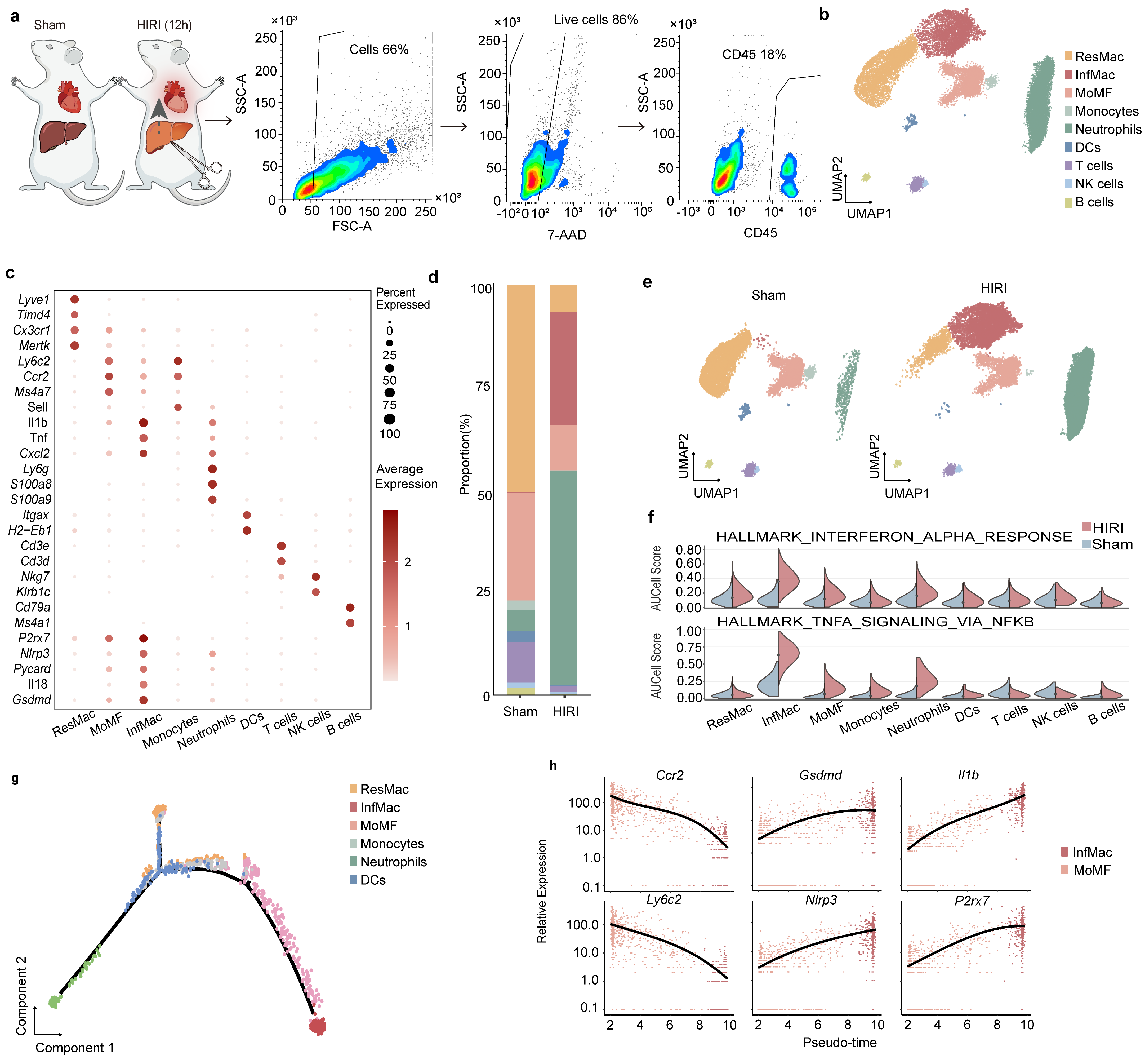
Single-cell sequencing reveals MoMF transition into P2X7-enriched inflammatory macrophages after HIRI
Functional validation localized the gating step to macrophage-side P2X7. Macrophage depletion attenuated HIRI-induced cardiac dysfunction. Side-specific siRNA knockdown showed that macrophage P2X7 ablation suppressed downstream cardiomyocyte GSDMD pyroptosis, whereas cardiomyocyte-side P2X7 knockdown did not. Cardiac macrophages thus function as amplifiers of liver-derived danger signals. To evaluate therapeutic strategies, the team tested two complementary purinergic interventions. The selective P2X7 antagonist JNJ-47965567 preserved cardiac function when administered within approximately three hours after reperfusion onset, with efficacy declining at six hours. Adenosine attenuated cardiac injury in a dose-dependent manner via the A2A receptor and conferred greater protection than dexamethasone or N-acetylcysteine under matched conditions, supporting pathway-specific purinergic intervention as a translational direction.
The work advances perioperative organ protection in three respects. It provides the first quantitative clinical link between hepatic and cardiac injury, offering a new basis for risk stratification in patients undergoing hepatic surgery. It defines a complete molecular cascade from circulating DAMPs to cardiac macrophage P2X7-NLRP3 to cardiomyocyte GSDMD pyroptosis, positioning cardiac macrophages as amplifiers of remote organ danger signals. It identifies the ATP-P2X7 and adenosine-A2A axes as complementary therapeutic targets with a defined pharmacological window, supporting translation toward pathway-specific perioperative cardioprotection.
The study, titled “Circulating ATP from hepatic ischemia-reperfusion drives remote cardiac injury via macrophage inflammasome activation,” was published online in Pharmacological Research (Impact Factor 12.2, JCR Q1 Top). Prof. Zhifeng Gao serves as the sole corresponding author, with Beijing Tsinghua Changgung Hospital as the lead corresponding institution. Zheng Zhang (Tsinghua University doctoral candidate) and Dr. Yi Duan (Associate Chief Physician, Department of Anesthesiology) are co-first authors. Doctoral candidates Fulei Gu, Jinyan Wei, and Hongyu Huo, and master’s student Yuze Wang also contributed substantially to the work. The authors gratefully acknowledge Prof. Dan Lu of the Institute of Systems Biomedicine, Peking University, for invaluable guidance throughout study design and manuscript preparation.
Sequencing data have been deposited in the NGDC Genome Sequence Archive (BioProject PRJCA056221).
DOI: https://doi.org/10.1016/j.phrs.2026.108306












 Research Updates
Research Updates